M.Bhuvana phanindra
Hallticket no:1701006100.
A 28year old female presented to casualty with complaints of
-headache since 3 days,
-Fever since 3 days,
-Decreased appetite since 3 days .
History of presenting illness:

Patient was apparently asymptomatic 8 days back later she ingested rodenticide (zinc phosphide) of aprroximatly:12-14grms
After ingestion ; two episodes of vomiting, abdominal pain , difficulty in speech and altered behaviour. Was treated for the same.
3 days back she developed generalized headache, no aggrevating and reliving factors, fever continuous low grade type ,not associated with chills and rigors. Associated with decreased appetite.
No history of loss of consciousness, seizures, sob , involuntary defecation and micturition.
No history of Loose stools.
Past history:
No similar complaints in the past.
Not a know case of DM, HTN, TB, asthama, or any other chronic illness.
Personal history:
Appetite: decreased
Diet :mixed
Bowel and bladder : regular
Sleep : adequate.
No addictions.
General examination:
patient was conscious, coherent, cooperative, oriented to time, place and person.
No pallor, icterus ,cyanosis ,clubbing, koilynchia lymphadenopathy ,edema.
Vitals:
Temperature:100°F
Pulse rate: 100bpm
Respiratory rate: 15cpm
Blood pressure: 110/80mmhg
Spo2 at room air: 97%
GRBS: 133mg%
Systemic examination:
CNS:
Level of consciousness: drowsy but arousable
Speech: aphasic
No meningeal signs
Glassgowcoma scale: E4,V1,M6. (11/15).
CVS: S1 S2 heard, apex beat-normal, no murmurs and bruits.
Respiratory system: bilateral air entry present, normal vescular breath sounds heard.
Per abdomen: soft, nontender, no organomegaly.
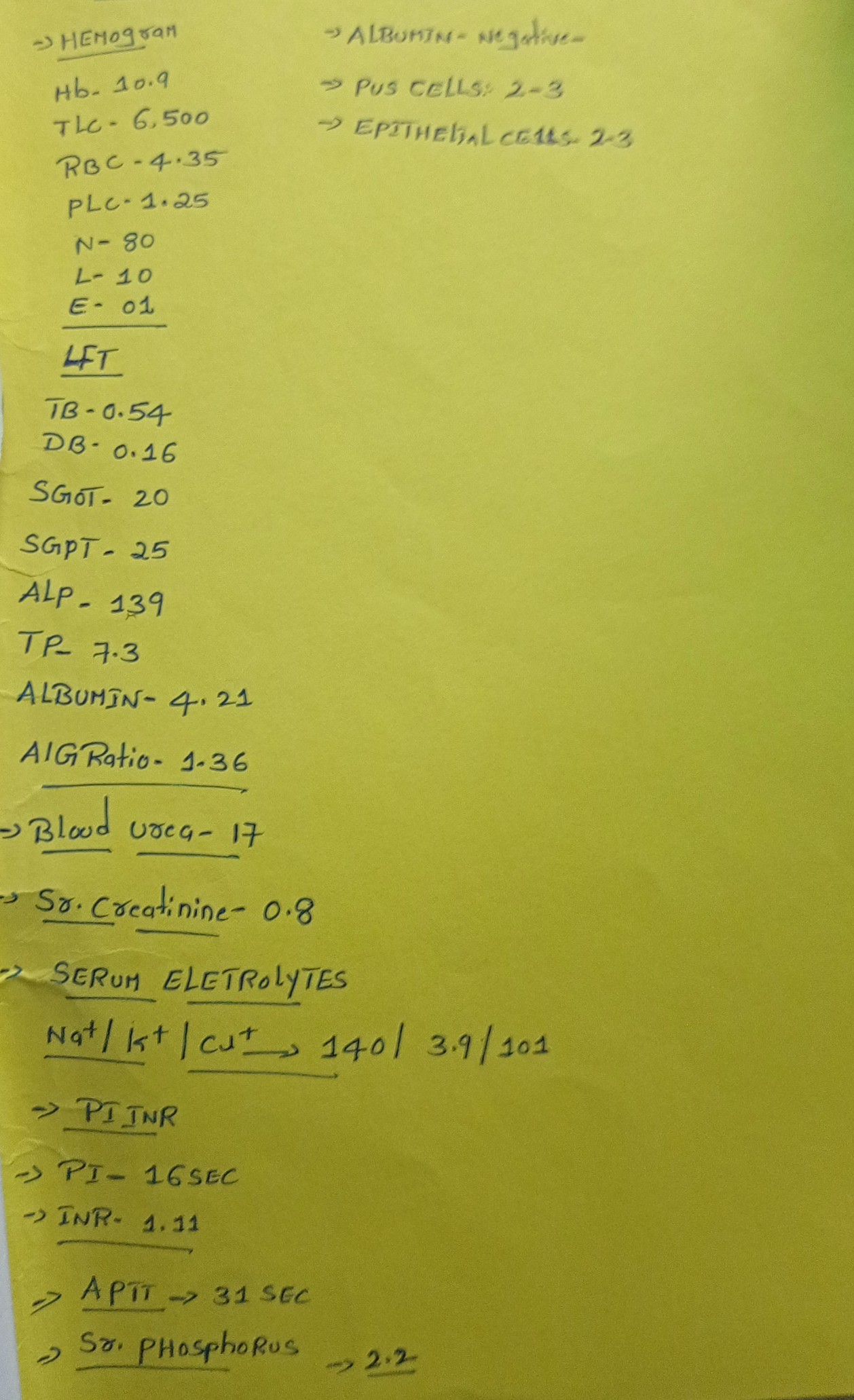
Investigations:
Deranged pt , aptt .

Provisional diagnosis:
Zinc phosphide poisioning. (Rodenticide)
Management:
Regular monitoring of vitals
1.INJ NAC 50MG/KG IN 500ML DNS
2.INJ PANTAPRAZOLE 40MG IV/OD
3.INJ ONDENSETRON 4MG Iv/OD
4.INJ NAC 1GM IV/OD
5.INJ VIT K 10MG IM STAT
6.CAP EVION 400MG PO OD
7. INJ SODIUM BICARBONATE 50MEQ /IV/STAT
8. INJ.SODA BICARB 1MEQ/KG/HR/IV
9. INJ.FUROSEMIDE 20MG/IV/BD
10. SYP SUCRALFATE 10ML POTID
11 .OPTINEURON 1 AMPOULE IN 500ML NS


Comments
Post a Comment